

Transplant transport
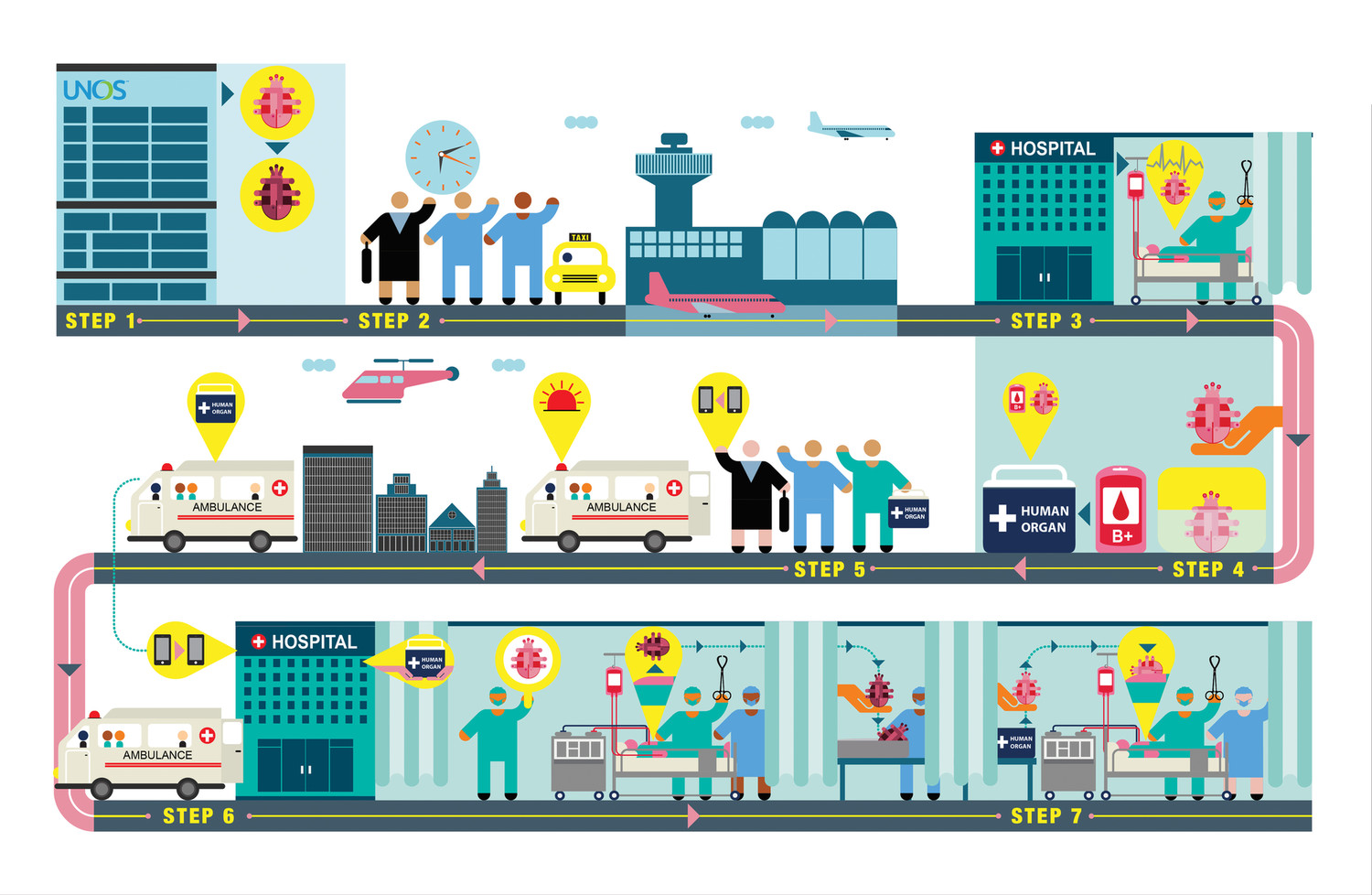
For each heart transplant surgery, getting the donor heart to the operating room in the best possible condition is a finely rehearsed relay race
Procuring and transporting a human heart for transplant is a race.
Once the beating heart of a brain-dead donor is stopped and removed, its cells begin to show stress from lack of oxygen. After too long, the heart can no longer be revived.
Time out of body—“ischemic time”—is best kept to under four hours. “We try to avoid greater than six hours,” says University of Minnesota Health cardiologist Cindy Martin, M.D.
That’s not much time to remove an organ, get it to the recipient, and complete a complicated transplant surgery. Plus, not everyone is a suitable donor. Most are younger than 55, have no history of chest trauma or cardiac disease, and have a normal electrocardiogram and echocardiogram.
These limitations mean fewer hearts for fewer people. In 2017, 3,244 hearts were transplanted in the United States. But more than 100,000 patients could benefit from a new heart, Martin says.
University of Minnesota Health surgeons transplant about 30 hearts each year. And with each surgery, the transplant teams go through a finely rehearsed relay race to ensure that every available heart gets to the operating room in the best possible condition.
Click on the numbers below to find out how a donor heart gets to its recipient.
ILLUSTRATION BY INFOMEN
More hearts for more people
A new organ transportation device being evaluated through clinical trials at the University of Minnesota and several other major heart transplant centers stands to make more hearts available to the people who need them.
The device is the TransMedics Organ Care System (OCS), often called the “heart in a box.” The machine, not much larger than a rolling suitcase, perfuses a warm, beating donor heart with oxygenated blood as it is being transported to the operating room. TransMedics donated machines to the University for the study.
The device could have a “huge impact” on the donor organ allocation system, says Kenneth Liao, M.D., Ph.D., surgical director of the University of Minnesota Health heart transplantation program and professor of surgery in the Medical School.
By keeping the heart in better condition longer, procurement teams can travel farther to retrieve a heart. And by monitoring the heart during transport, the OCS allows surgeons to test a “suboptimal” heart they otherwise wouldn’t risk using.
“That would open the door for a lot of organs that potentially would be rejected by the transplant centers,” Liao says, “and that would increase the volume of the donor pool.”







-2.jpg?w=1100)