

The changing demographics of colorectal cancer
M Health Fairview colorectal surgeon Genevieve Melton-Meaux, M.D., Ph.D., explains why screening colonoscopies are now recommended starting at age 45
Colorectal cancer is not strictly an older person’s disease. Rates of colon cancer are steadily rising among younger Americans, prompting a shift in the recommended age for a person’s first screening colonoscopy from age 50 to 45.
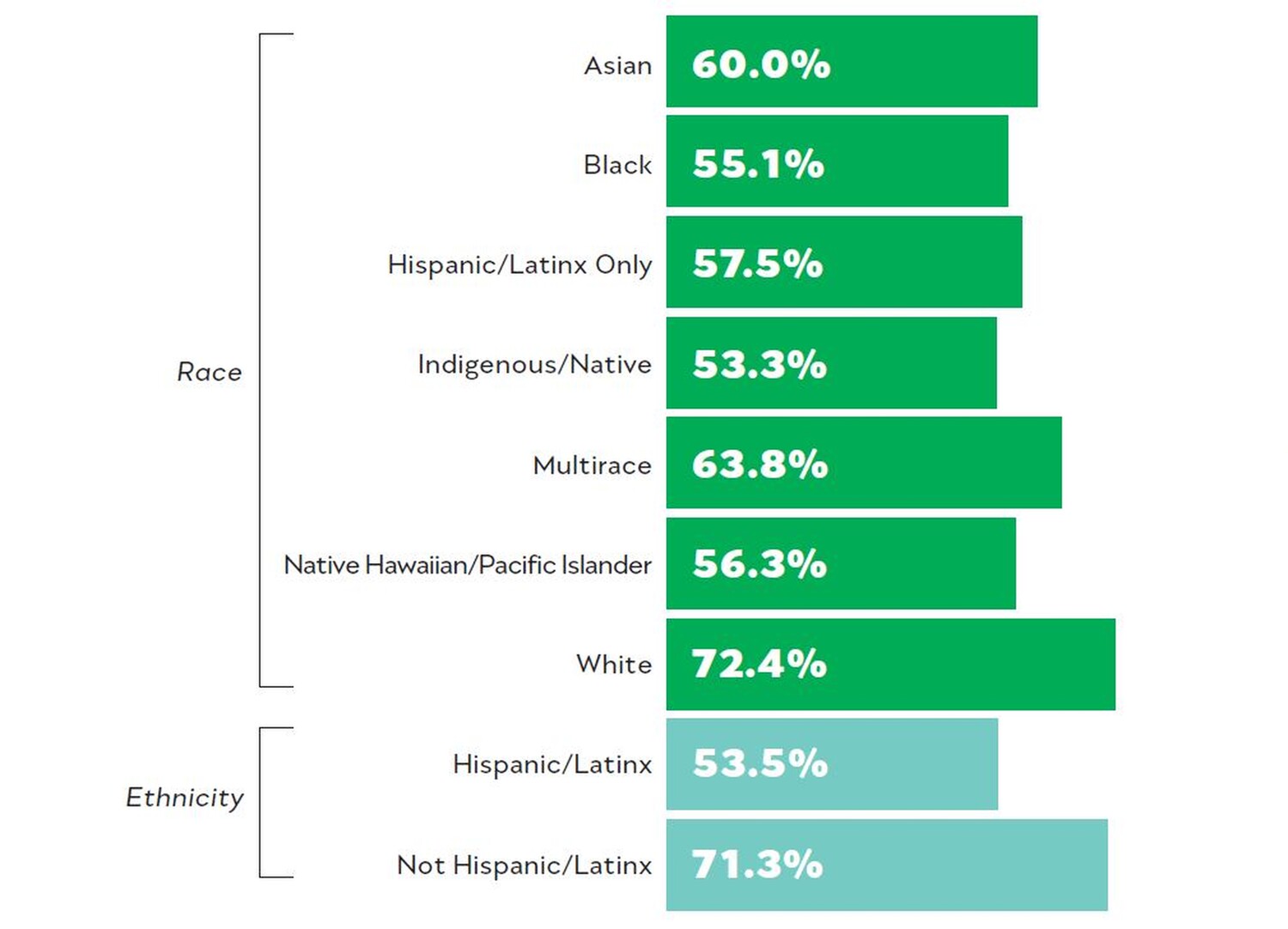
Researchers also are seeing that Black Americans are 20% more likely to get colorectal cancer—and 40% more likely to die from it—than people in other racial or ethnic groups. In Minnesota, American Indians are at a dramatically higher risk of having colon cancer and dying from it, too.

M Health Fairview colon and rectal surgeon Genevieve Melton-Meaux, M.D., Ph.D., who is also the health system’s chief analytics and care information officer as well as a professor of surgery in the University of Minnesota Medical School and member of the Masonic Cancer Center, talks about what’s going on and how she and her colleagues are working to prevent colon cancer deaths across all our communities.
What’s causing the shift in who’s developing colorectal cancer?
A lot of it has to do with diet. Some of it is [geography], and some is genetics; some families that are high risk need much more frequent screening. I think this has happened gradually over time, and finally the data was convincing. It’s clear we need to start screening earlier.
Why is early detection so important?
With stage 1 cancer, the chances of having long-term disease are in the 5% range. When colon cancer has spread to the lymph nodes, the rate of disease-free survival is about 40%. That means all these other treatments: [more invasive] surgery, and sometimes chemotherapy.
What are you and your colleagues doing to get more people screened?
We’ve put together a proactive outreach approach, where we’re not only calling patients but also putting alerts out. One way is through the patient portal chart. And we’re about to launch a campaign where we’re going to be text-messaging patients.
Through a different program, we’re reaching people as soon as they need to be screened—and for people at higher risk, we’re holding onto them tighter. If you come in for a colonoscopy and you have a polyp, instead of following up at 10 years, we’re [urging] you to follow up at five years. Or three. Or in some cases, even one year. We work with some community groups on outreach activities, too—for instance, in [predominantly] African American churches.
How are these new approaches better than the status quo?
We need to do better at personalizing it to the individual: understanding what their motivations are, what barriers they face. We can’t just improve overall: we have to look at the equity aspects of what we’re doing, and improve in the populations that are behind.






-2.jpg?w=1100)
