

Need a doctor? We can help
The Medical School’s Mark Rosenberg, M.D., talks about what it will take to fill Minnesota’s physician shortage

We’re on the verge of a health care crisis, and this one isn’t COVID-19: it’s a nationwide shortage of physicians.
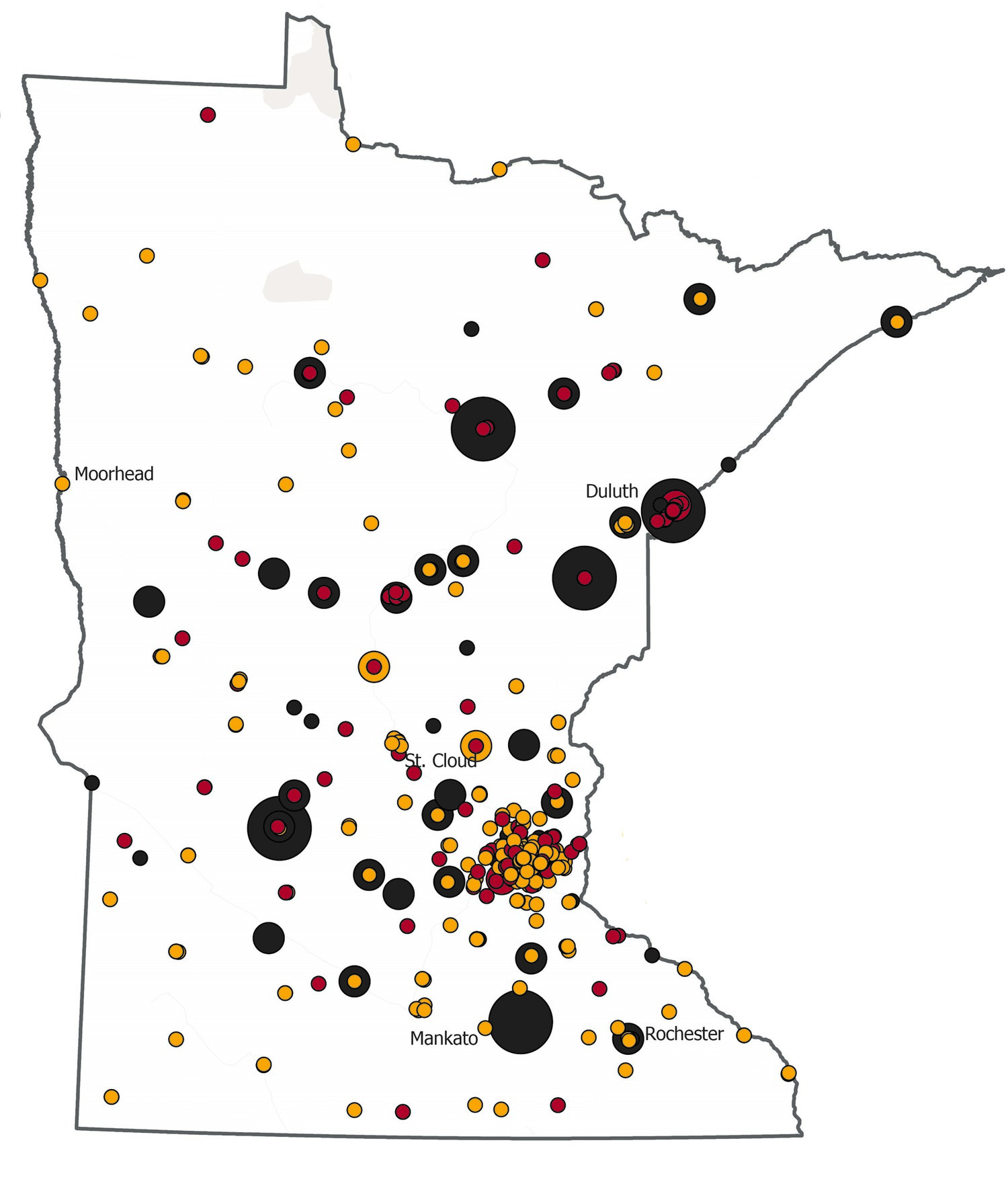
Here in Minnesota, the provider shortage is more pronounced in rural areas—where half our state’s population resides but only about 12% of our physicians practice.
University of Minnesota Medical School vice dean of education and academic affairs Mark Rosenberg, M.D., and his colleagues are tackling that problem by making changes in what medical education looks like.
And because about 70% of Minnesota’s health care providers train at the University of Minnesota, they have a chance to make a big impact.
How do we get more doctors to choose rural medicine or primary care?
We’re designing education to match the workforce needs of Minnesota and beyond. One example program is RPAP, our Rural Physician Associate Program. (See below.) Students who enter this program are much more likely to practice in rural settings, to practice primary care and specifically family medicine, and to stay in Minnesota.
We’re already doing really well here, if you look at the national numbers. Our Medical School is first in the country for producing family physicians, third for producing rural physicians, and fifth for producing primary care physicians.
How do you prepare medical students to eventually fill these important roles, especially when they might be the only physician in town?
Knowledge in medicine is exploding at such a huge rate that it’s impossible to teach or learn everything. We want our students to develop skills for lifelong learning. How can they access information when they need it? How can they understand clinical practice guidelines to improve outcomes?
We’re also emphasizing the importance of being effective interprofessional team members—to work with nurses, social workers, and pharmacists. So even in a small practice, they’re never really alone.
How do you know they’re ready?
We now evaluate students on 13 outcomes called “entrustable professional activities”—work that a doctor does, like performing a physical, taking a medical history, ordering tests, recognizing when someone is very sick and needs immediate attention. It helps learners know where they are along the continuum to becoming independent practitioners. You can see the curves of improvement as they do more.
How do you attract the students who will become the best physicians?
Sometimes it comes down to scholarships. Medical school is expensive. The average debt of a medical student here is in the $180,000 range.
There’s some evidence that student debt can drive future career choices. Medical specialists who work in metropolitan areas have higher salaries than family physicians working outstate or in underserved urban areas. Scholarships free students up by offsetting their debt, so their choice is not so much about their future earning potential and paying off their debt as it is about their passions.





-2.jpg?w=1100)