

How racism affects your health
Brooke Cunningham, M.D., Ph.D., addresses racial disparities, provider bias, and how we can make meaningful change
“Can’t you just work on something else?” It’s a question that Brooke Cunningham, M.D., Ph.D., has fielded repeatedly.
An assistant professor in the University of Minnesota Medical School’s Department of Family Medicine and Community Health, Cunningham studies racial inequities in health and health care systems, and providers’ willingness to address racism as the fundamental cause.
Historically, it hasn’t been easy to fund this work, making an uphill battle even more difficult.

Today Cunningham is designing a framework for health care providers—and specifically white providers—to talk with their patients about their experiences living in a Black or brown body. She hopes this will have a healing effect for patients and a positive effect on providers as well.
“We want to provide the best possible care for people of color,” says Cunningham, who sees patients at the Community-University Health Care Center in Minneapolis, “and it’s hard for me to think about doing that without exploring patients’ exposure to racism.”
Minnesota consistently ranks among the country’s healthiest states but also has some of the worst health disparities. How did we get here?
Many of our social systems, from their inception, were designed to benefit white Minnesotans. We are dealing with their legacies of exclusion.
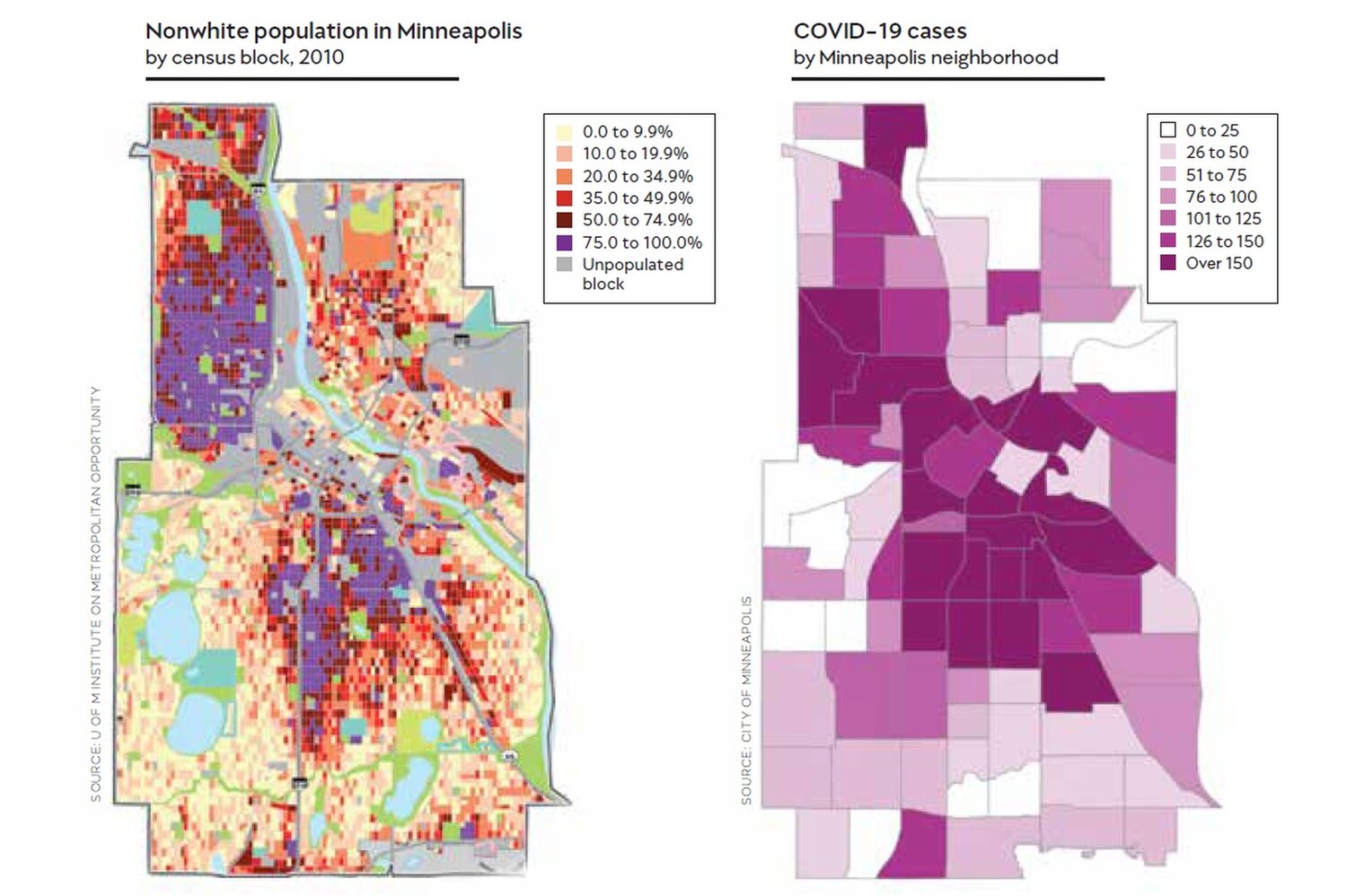
For example, the Twin Cities are still very segregated. Black people who live in more segregated cities have poorer health outcomes, because segregation is associated with school quality, neighborhood amenities, green space, alcohol and tobacco marketing, and, most importantly, concentrated poverty.
We Minnesotans like to think of ourselves as “nice.” This doesn’t sound very nice at all.
It’s hard for people to accept. It seems paradoxical. It makes me wonder if “Minnesota nice” or our belief in our own progressivity could actually be obstacles to furthering racial equity.
How do we make meaningful change going forward?
We look at overtly racist groups, like white nationalists, and say, “They’re hateful. That’s not me.” But that definition of racism is not the definition we need to work with.
Racism is a system that differentially advantages and conversely disadvantages people based on racial group membership. If you are antiracist, you have to actively support policies that work to upend racial privilege. That means if a policy or practice has a disproportionately negative impact on Blacks, Indigenous people, or other people of color, we change that policy—even when nobody’s watching or it’s inconvenient or it comes at some cost to us personally.
What role can philanthropy play in accelerating progress?
What every researcher most wants is flexible capital. That gives us the discretion to be creative and adapt when there are new ideas.
In addition, to the extent that philanthropy can extend my networks, new connections would be really meaningful to me. I have often felt isolated in this work, even though I know that there are a lot of people who care about racial justice. I don’t want to be on my ship alone.
Make a gift to support health equity by contacting Sarah Barsness of the University of Minnesota Foundation at 612-625-5976 or sbarsnes@umn.edu.

.jpg?w=1100)




-2.jpg?w=1100)
